
Cardiac stimulation: fibrillation
Electromedical equipment is a possible source of hazard to the patient. In many cases the patient is directly connected to the equipment so that in cases of a fault electrical current may flow through the patient. The response of the body to low-frequency alternating current depends on the frequency and the current density. Low-frequency current (up to 1 kHz) which includes the main commercial supply frequencies (50 Hz and 60 Hz) can cause: prolonged tetanic contraction of skeletal and respiratory muscles; arrest of respiration by interference with the muscles that control breathing; heart failure due to ventricular fibrillation (VF). In calculating current through the body, it is useful to model the body as a resistor network. The skin can have a resistance as high as 1 M (dry skin) falling to 1 k (damp skin). Internally, the body resistance is about 50. Internal conduction occurs mainly through muscular pathways. Ohm’s law can be used to calculate the current. For example, for a person with damp skin touching both terminals of a constant voltage 240 V source (or one terminal and ground in the case of mains supply), the current would be given by I = V /R = 240/2050 = 117 mA, which is enough to cause ventricular fibrillation (VF).
Indirect cardiac stimulation
Most accidental contact with electrical circuits occurs via the skin surface. The threshold of current perception is about 1 mA, when a tingling sensation is felt. At 5 mA, sensory nerves are stimulated. Above 10 mA, it becomes increasingly difficult to let go of the conductor due to muscle contraction. At high levels the sustained muscle contraction prevents the victim from releasing their grip. When the surface current reaches about 70–100 mA the co-ordinated electrical control of the heart may be affected, causing ventricular fibrillation (VF).
The fibrillation may continue after the current is removed and will result in death after a few minutes if it persists. Larger currents of several amperes may cause respiratory paralysis and burns due to heating effects. The whole of the myocardium contracts at once producing cardiac arrest. However, when the current stops the heart will not fibrillate, but will return to normal co-ordinated pumping. This is due to the cells in the heart all being in an identical state of contraction. This is the principle behind the defibrillator where the application of a large current for a very short time will stop ventricular fibrillation.
The VF threshold varies in a similar way; currents well above 1 kHz, as used in diathermy, do not stimulate muscles and the heating effect becomes dominant. IEC 601-1 limits the AC leakage current from equipment in normal use to 0.1 mA.
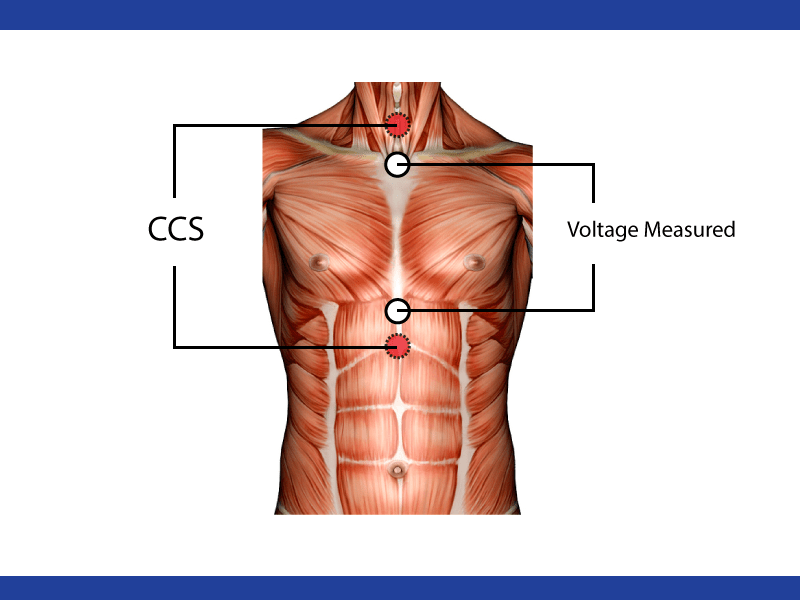
Direct cardiac stimulation
Currents of less than 1 mA, although below the level of perception for surface currents, are very dangerous if they pass internally in the body in the region of the heart. They can result in ventricular fibrillation and loss of pumping action of the heart.
Currents can enter the heart via pacemaker leads or via fluid-filled catheters used for pressure monitoring. The smallest current that can produce VF, when applied directly to the ventricles, is about 50 μA. British Standard BS5724 limits the normal leakage current from equipment in the vicinity of an electrically susceptible patient (i.e. one with a direct connection to the heart) to 10 μA, rising to 50 μA for a single-fault condition.
Note that the 0.5 mA limit for leakage currents from normal equipment is below the threshold of perception. but above the VF threshold for currents applied to the heart. Percentage of adult males who can ‘let go’ as a function of frequency and current.
Ventricular fibrillation VF occurs when heart muscle cells coming out of their refractory period are electrically stimulated by the fibrillating current and depolarize, while at the same instant other cells, still being in the refractory period, are unaffected. The cells depolarizing at the wrong time propagate an impulse causing other cells to depolarize at the wrong time. Thus, the timing is upset and the heart muscles contract in an unco-ordinated fashion. The heart is unable to pump blood and the blood pressure drops. Death will occur in a few minutes due to lack of oxygen supply to the brain. To stop fibrillation, the heart cells must be electrically co-ordinated by use of a defibrillator.
The threshold at which VF occurs is dependent on the current density through the heart, regardless of
the actual current. As the cross-sectional area of a catheter decreases, a given current will produce increasing current densities, and so the VF threshold will decrease.
HIGHER FREQUENCIES: >100 kHz
Surgical diathermy/electrosurgery
Surgical diathermy/electrosurgery is a technique that is widely used by surgeons. The technique uses an electric arc struck between a needle and tissue in order to cut the tissue. The arc, which has a temperature in excess of 1000 ◦ C, disrupts the cells in front of the needle so that the tissue parts as if cut by a knife; with suitable conditions of electric power the cut surfaces do not bleed at all. If blood vessels are cut these may continue to bleed and current has to be applied specifically to the cut ends of the vessel by applying a blunt electrode and passing the diathermy current for a second, or two or by gripping the end of the bleeding vessel with artery forceps and passing diathermy current from the forceps into the tissue until the blood has coagulated sufficiently to stop any further bleeding. Diathermy can therefore be used both for cutting and coagulation.
The current from the ‘live’ or ‘active’ electrode spreads out in the patient’s body to travel to the
‘indifferent’, ‘plate’ or ‘patient’ electrode which is a large electrode in intimate contact with the patient’s body. Only at points of high current density, i.e. in the immediate vicinity of the active electrode, will coagulation take place; further away the current density is too small to have any effect. Although electricity from the mains supply would be capable of stopping bleeding, the amount of
current needed (a few hundred milliamperes) would cause such intense muscle activation that it would be impossible for the surgeon to work and would be likely to cause the patient’s heart to stop. The current used must therefore be at a sufficiently high frequency that it can pass through tissue without activating the muscles.
Diathermy equipment
Diathermy machines operate in the radio-frequency (RF) range of the spectrum, typically 0.4–3 MHz.
Diathermy works by heating body tissues to very high temperatures. The current densities at the active electrode can be 10 A cm −2 . The total power input can be about 200 W. The power density in the vicinity of the cutting edge can be thousands of W cm −3 , falling to a small fraction of a W cm −3 a few centimetres from the cutting edge. The massive temperature rises at the edge (theoretically thousands of ◦ C) cause the tissue fluids to boil in a fraction of a second. The cutting is a result of rupture of the cells.
An RF current follows the path of least resistance to ground. This would normally be via the plate (also called dispersive) electrode. However, if the patient is connected to the ground via the table or any attached leads from monitoring equipment, the current will flow out through these. The current density will be high at these points of contact, and will result in surface burns (50 mA cm −2 will cause reddening of the skin; 150 mA cm −2 will cause burns). Even if the operating table is insulated from earth, it can form a capacitor with the surrounding metal of the operating theatre due to its size, allowing current to flow. Inductive or capacitive coupling can also be formed between electrical leads, providing other routes to ground.
Heating effects
If the whole body or even a major part of the body is exposed to an intense electromagnetic field then the heating produced might be significant. The body normally maintains a stable deep-body temperature within relatively narrow limits (37.4 ± 1 ◦ C) even though the environmental temperature may fluctuate widely. The normal minimal metabolic rate for a resting human is about 45 W m −2 (4.5 mW cm −2 ), which for an average surface area of 1.8 m 2 gives a rate of 81 W for a human body. Blood perfusion has an important role in maintaining deep-body temperature. The rate of blood flow in the skin is an important factor influencing the internal thermal conductance of the body: the higher the blood flow and hence, the thermal conductance, the greater is the rate of transfer of metabolic heat from the tissues to the skin for a given temperature difference.
Blood flowing through veins just below the skin plays an important part in controlling heat transfer. Studies have shown that the thermal gradient from within the patient to the skin surface covers a large range and gradients of 0.05–0.5 ◦ C mm −1 have been measured. It has been shown that the effect of radiation emanating from beneath the skin surface is very small. However, surface temperatures will be affected by vessels carrying blood at a temperature higher or lower than the surrounding tissue provided the vessels are within a few millimetres of the skin surface. Exposure to electromagnetic (EM) fields can cause significant changes in total body temperature. Some of the fields quoted in table 8.3 are given in volts per metre. We can calculate what power dissipation this might cause if we make simplifying assumptions, which represents a body which is 30 cm in diameter and 1 m long (L). We will assume a resistivity (ρ) of 5m for the tissue. The resistance (R) between the top and bottom will be given by ρL/A where A is the cross-sectional area. R = 70.7 For a field of 1 V m −1 (in the tissue) the current will be 14.1 mA. The power dissipated is 14.1 mW which is negligible compared to the basal metabolic rate. applied fielddiameter 30 cm length 100 cm resistivity assumed to be 5 ohm metre. The body modelled as a cylinder of tissue. For a field of 1 kV m −1 , the current will be 14.1 A and the power 14.1 kW, which is very significant.
The power density is 20 W cm −2 over the input surface or 200 mW cm −3 over the whole volume.
In the above case we assumed that the quoted field density was the volts per metre produced in tissue.
However, in many cases the field is quoted as volts per metre in air. There is a large difference between these two cases. A field of 100 V m −1 in air may only give rise to a field of 10 −5 V m −1 in tissue.
ULTRAVIOLET
We now come to the border between ionizing and non-ionizing radiation. Ultraviolet radiation is part of the electromagnetic spectrum and lies between the visible and the x-ray regions. It is normally divided into three wavelength ranges. These define UV-A, UV-B and UV-C by wavelength.
A 315–400 nm
B 280–315 nm
C 100–280 nm
The sun provides ultraviolet (mainly UV-A and UV-B) as well as visible radiation. Total solar irradiance is about 900 W m −2 at sea level, but only a small part of this is at ultraviolet wavelengths. Nonetheless there is sufficient UV to cause sunburn. The early effects of sunburn are pain, erythema, swelling and tanning. Chronic effects include skin hyperplasia, photoaging and pseudoporphyria. It has also been linked to the development of squamous cell carcinoma of the skin. Histologically there is subdermal oedema and other changes.
Of the early effects UV-A produces a peak biological effect after about 72 h, whereas UV-B peaks at
12–24 h. The effects depend upon skin type. The measurement of ultraviolet radiation Exposure to UV can be assessed by measuring the erythemal response of skin or by noting the effect on micro-organisms. There are various chemical techniques for measuring UV but it is most common to use
physics-based techniques. These include the use of photodiodes, photovoltaic cells, fluorescence detectors and thermoluminescent detectors such as lithium fluoride. Therapy with ultraviolet radiation Ultraviolet radiation is used in medicine to treat skin diseases and to relieve certain forms of itching. The UV radiation may be administered on its own or in conjunction with photoactive drugs, either applied directly to the skin or taken systemically.
The most common application of UV in treatment is psolaren ultraviolet A (PUVA). This has been
used extensively since the 1970s for the treatment of psoriasis and some other skin disorders. It involves the combination of the photoactive drug psoralen, with long-wave ultraviolet radiation (UV-A) to produce a beneficial effect. Psoralen photochemotherapy has been used to treat many skin diseases, although its principal success has been in the management of psoriasis. The mechanism of the treatment is thought to be that psoralens bind to DNA in the presence of UV-A, resulting in a transient inhibition of DNA synthesis and cell division. 8-methoxypsolaren and UV-A are used to stop epithelial cell proliferation. There can be side effects and so the dose of UV-A has to be controlled. Patch testing is often carried out in order to establish what dose will cause erythema. This minimum erythema dose (MED) can be used to determine the dose used during PUVA therapy.
In PUVA the psoralens may be applied to the skin directly or taken as tablets. If the psoriasis is
generalized, whole-body exposure is given in an irradiation cabinet. Typical intensities used are 10 mW cm −2 , i.e. 100 W m −2 . The UV-A dose per treatment session is generally in the range 1–10 J cm −2 . Treatment is given several times weekly until the psoriasis clears. The total time taken for this to occur will obviously vary considerably from one patient to another, and in some cases complete clearing of the lesions is never achieved. PUVA therapy is not a cure for psoriasis and repeated therapy is often needed to prevent relapse.



_PRIME.svg)























.png)



![v={\frac {\Gamma }{4\pi r}}\left[\cos A-\cos B\right]](https://wikimedia.org/api/rest_v1/media/math/render/svg/a637f2184bebca871053d36b0e621c88211386d9)